ALTERED SENSORIUM SECONDARY TO ? HYPONATREMIA(RESOLVED)WITH ALCOHOL WITHDRAWAL SEIZURE(RESOLVED)WITH PYREXIA SECONDARY TO UTI
*ICU Admission under unit-6*
Under the guidance of DR.VAISHNAVI MAM AND DR.MANASA MAM
45 yr old Male came to casuality with chief complaints of Fever since 2 days in Drowsy state..
Fever - High grade, intermittent, associated with chills
HOPI+ pt was apparently asymptomatic 6 days ago, later he developed
vomitings-1 to 5 episodes/day, non bilious, non projectile, non blood tinged for which he went to a govt hospital & got treated...
Prior to vomitings pt had intake of alcohol (360ml)
2 days after he had involuntary movements of both upper & tower Limbs (? Generalized tonic clonic seizures) - 1episode, which is associated with froathing, tongue bite..
pt was unconscious during this episode. He was taken to a private hospital & managed conservatively
2 days back patient was conscious & coherent, talking but he is in drowsy state.
Patient stopped working since 1 year (due to generalized weakness)
2 months back - pt had back pain (occasionally taken pain killers).
H/O alcohol consumption since 15yrs(weekly thrice)
Zarda pan consumption - since 15 years Daily 1pack.
No H/O smoking
Not a k/c/o DM, HTN, Asthma,TB, CAD
No H/o any past surgeries
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
Afebrile
PR: 108 bpm, regular
RR: 26 cpm
BP: 80/50 mmHg
SPO2:
AT ROOM AIR-96%
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
Pt obeying motor commands
E4V5M6
Power-(4/5. 4/5)
Tone-(normal. Normal)
*PROVISIONAL DIAGNOSIS-*
Altered sensorium secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure(resolved)
With pyrexia secondary to UTI



Psychiatry refferal was taken
Here is their notes
A 45 year old patient farmer by occupation was presented to the Casualty with chief complaint of altered sensorium since 1 week secondary to hyponatremia?? Alcohol withdrawal??
History of present illness:
Patient was apparently asymptomatic 1 week back before standing illness.Then the patient was admitted to casualty on 18/09/2021 complaining of altered sensorium.
Patient had hyponatremia with history of alcohol withdrawal and seizures with alcohol and tobacco dependence.
According to the patient's wife, patient consumes alcohol 12 units twice a week since 10 years.
1 year back patient had an injury to his back under the influence of alcohol when he was asked to stop alcohol consumption completely because of jaundice.since then patient didn't consume alcohol until 10/09/2021 when he consumed alcohol.Patient had vomitings of 2 to 3 episodes at 2 o'clock that night (according to his wife) and also Chills and febrile for which he was taken to nearer hospital.I.V fluids and medications are given for the same.Symptoms got reduced on taking medications.
But it has recurred on 12/09/2021 where he was to nalgonda govt hospital.
On 12/09/2021 night patient threw seizures (Tonic clonic seizures) for the first time, with tongue bite as per patient's wife.Post ictal confusion was present. Since then patient was weak and drowsy after the episode of seizures.As they found patient was not improving he was shifted to some private hospital.There treatment was given treatment for dyselectrolytemia. Patient was improved in 3 -4 days but again started deteriorating from 18/09/202 morning.Patient was advised for imaging and was asked to take patient to higher center, so was admitted to our hospital on 18/09/202 at 4 pm
Patient had a habit of chewing tobacco once in 3 days.
Patient had sleep disturbances, cravings and tremors if he doesn't consume alcohol and tobacco.
On presentation:
Patient is Thin built and shivering at times.
Patient was lying in fetal position.
Opening eyes on calling his name.
According to history of patient having spikes of fever along with confusion and drowsiness.
Need of ruling out causes for seizures and altered sensorium.
No H/o other substance use.
No H/o head injury.
No H/o self talking,self smiling.
No H/o pervasive low mode suicidality.
No H/o repetitive thoughts and actions.
No H/o blood in vomitus and stool.
No significant H/o psychiatric history in family.
Past history
No history of DM/HTN/Epilepsy/TB/Thyroid disorders
The patient had not undergone any surgeries.
Personal history
Diet : mixed
Appetite : normal (according to patient's wife)
Bowel and bladder : normal
Sleep : disturbances
Addictions: pan since 15 years daily 1 pack and alcohol consumption since 15 years weekly thrice.No history of smoking.
Family history
No history of DM/HTN/CVA/CAD/Asthma/thyroid disorders
No similar complaints in the family previously.
Treatment history
Not significant.
General examination
Patient is conscious but drowsy.
Oriented to person only.
No pallor, history of icterus previously but not now,no cyanosis,no clubbing,no lymphadenopathy.


By DR.RAGHUNATH PG1 PSYCHIATRY DEPARTMENT(MAIN AUTHOR)
Psychiatry Notes typed by-Dr.Ramya BDS UG

ON DAY 4-NIGHT
BP MONITORING
9pm-100/60mmhg
10pm-90/60mmhg
11pm-90/60mmhg
12am-90/60mmhg
1 am-90/60mmhg
2am-90/60mmhg
3 am-80/60mmhg
4am-70/60- Nor Ad-2 amp in 46ml NS@6ml/hr started
5am-80/60mmhg
6 am-90/60mmhg
7am-100/60mmhg
ALSO HE HAD FEVER FROM 9 PM TO 1 AM
AS PATIENT'S BP GOT FLUCTUATIONS
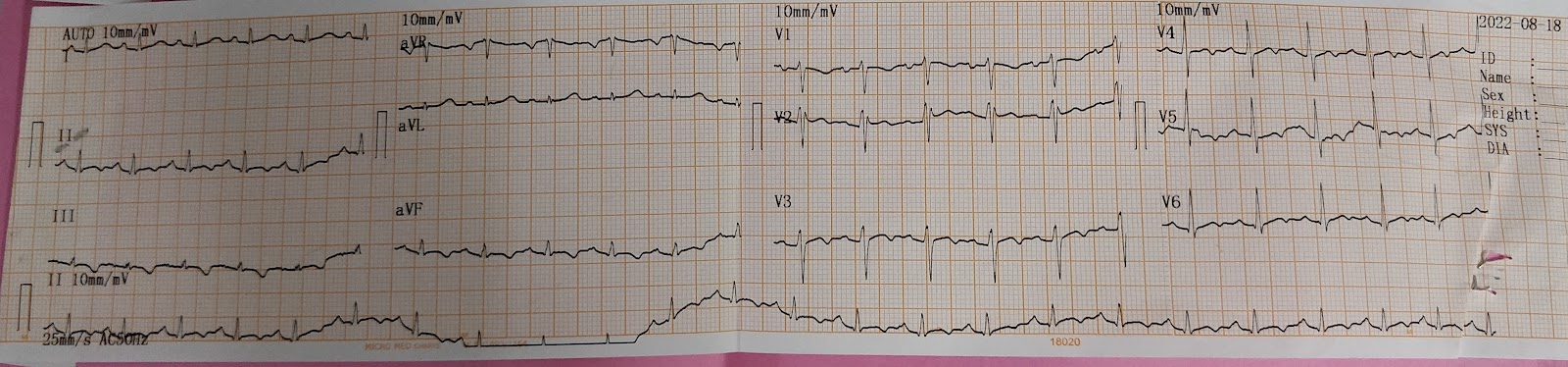
IN THE NIGHT, THE NEXT DAY ECG AND 2D ECHO WAS REPEATED
On day 5

T wave inversions in all leads
Therefore 2d echo was taken.Its mostly because of ionotropes withdrawal
(Cardiopathy ass with alcohol consumption)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2644041/
2d echo

On day 7 As his fever spikes continued
Repeated chest x ray to rule out pneumonia

Did usg abdomen to rule out liver abcess

Day 9
Ecg was repeated

Day 10 -Planning for discharge

Subjective-
2 episodes of fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
Afebrile
PR: 108 bpm, regular
RR: 18 cpm
BP: 80/50 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:81 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A:soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
Pt obeying motor commands
E4V5M6
Power-(4/5. 4/5)
Tone-(normal. Normal)
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia ?Alcohol withdrawal
Plan of care-
*1.RT FEEDS* -
100ml water -1 hourly
200ml milk with protein powder-2nd hourly
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.Levipil 500mg iv/bd
7.Inj.ceftriazone 2Gm iv/bd
8.W/F seizure episode
9.Monitor vitals-4rth hourly
10.I/O charting
SOAP NOTES DAY 2
Subjective-
2 episodes of fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
Afebrile
PR: 98 bpm, regular
RR: 19 cpm
BP: 100/60 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:116 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
Pt obeying motor commands
E4V5M6
Power-(4/5. 4/5)
Tone-(normal. Normal)
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia ?Alcohol withdrawal
Plan of care-
*1.RT FEEDS* -
100ml water -1 hourly
200ml milk with protein powder-2nd hourly
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.Levipil 500mg iv/bd
7.Inj.ceftriazone 2Gm iv/bd
8.W/F seizure episode
9.Monitor vitals-4rth hourly
10.I/O charting
SOAP NOTES DAY 3
Subjective-
2 episodes of fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
Afebrile
PR: 99 bpm, regular
RR: 20 cpm
BP: 100/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:81 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
Pt obeying motor commands
E4V5M6
Power-(4/5. 4/5)
Tone-(normal. Normal)
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia ?Alcohol withdrawal
Plan of care-
1.IV fluids
500ml RL
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.Levipil 500mg iv/bd
7.Inj.ceftriazone 2Gm iv/bd
8.W/F seizure episode
9.Monitor vitals-4rth hourly
10.I/O charting
SOAP NOTES DAY 4
Subjective-
1 episode of fever spike
Burning micturation+
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
Afebrile
PR: 78 bpm, regular
RR: 20 cpm
BP: 120/70 mmHg with NA@2ml/hr
SPO2:
AT ROOM AIR-98%
GRBS:112 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia ?Alcohol withdrawal
Plan of care-
1.IV fluids
500ml RL
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.Levipil 500mg iv/bd
7.Inj.cetriazone 2Gm iv/bd
8.Inj.Lorazepam2 cc IV/sos (if seizure episode)
9.Tab.Dolo650mg po/tid
10.Monitor vitals-4rth hourly
I/O charting
SOAP NOTES DAY 5
Subjective-
3 episodes of fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
BP MONITORING
yesterday
9pm-100/60mmhg
10pm-90/60mmhg
11pm-90/60mmhg
12am-90/60mmhg
1 am-90/60mmhg
2am-90/60mmhg
3 am-80/60mmhg
4am-70/60- Nor Ad-2 amp in 46ml NS@6ml/hr started
5am-80/60mmhg
6 am-90/60mmhg
7am-100/60mmhg
Vitals:
Afebrile
PR: 88 bpm, regular
RR: 20 cpm
BP: 100/60 mmHg with NA@6ml/hr
SPO2:
AT ROOM AIR-98%
GRBS:123 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure
With refractory hypotension
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
Monitor vitals-4rth hourly
I/O charting
SOAP NOTES DAY 6
Subjective-
2 episodes of fever spikes
Pt Is c/c/c
Oriented to t/p/p
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP-Afebrile
PR: 98 bpm, regular
RR: 20cpm
BP: 110/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:110mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure(resolved)
With pyrexia secondary to UTI
No fever spikes
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
8.Inj.Levipil 500mg iv/bd
9.Tab.Dolo650mg po/tid
10.Monitor vitals-4rth hourly
I/O charting
SOAP NOTES DAY 7
Subjective-
Continuous fever
Abdominal tenderness+
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
Afebrile
PR: 88 bpm, regular
RR: 20 cpm
BP: 70/50 mmHg with NA@6ml/hr
SPO2:
AT ROOM AIR-98%
GRBS:123 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium under evaluation secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure
With refractory hypotension
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
8.Inj.Levipil 500mg iv/bd
9.Tab.Dolo650mg po/tid
10.Monitor vitals-4rth hourly
I/O chartingSOAP NOTES DAY 8
Subjective-
No fever spikes
1 episode of vomiting yesterday
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP-100.3 F
PR: 102 bpm, regular
RR: 19cpm
BP: 100/60 mmHg with NA@4ml/hr
SPO2:
AT ROOM AIR-98%
GRBS:150mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure(resolved)
With pyrexia secondary to UTI
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
8.Inj.Levipil 500mg iv/bd
9.Tab.Dolo650mg po/tid
10.Monitor vitals-4rth hourly
I/O charting
SOAP NOTES DAY 9
Subjective-
No fever spikes
Pt Is c/c/c
Oriented to t/p/p
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP-Afebrile
PR: 98 bpm, regular
RR: 20cpm
BP: 110/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:110mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure(resolved)
With pyrexia secondary to UTI
No fever spikes
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
8.Inj.Levipil 500mg iv/bd
9.Tab.Dolo650mg po/tid
10.Monitor vitals-4rth hourly
I/O charting
SOAP NOTES DAY 10
Subjective-
No fever spikes
Pt Is c/c/c
Oriented to t/p/p
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP-Afebrile
PR: 95 bpm, regular
RR: 21cpm
BP: 110/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:110mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium secondary to ? Hyponatremia(resolved)
with alcohol withdrawal seizure(resolved)
With pyrexia secondary to UTI
No fever spikes
Plan of care-
1.IV fluids
0.9%NS@150ml/hr
2.Inj.pantop 40mg iv/OD
3.Inj.zofer 4 mg iv/sos
4.Inj.neomol 100ml iv/sos
(If temp is more than 101 degree F)
5.Inj.thiamine 100mg iv/tid
6.Inj.cetriazone 2Gm iv/bd
7.Inj.Lorazepam2 cc IV (if seizure episode)
8.Inj.Levipil 500mg iv/bd
9.inj.meropenam iv/Bd (day 4)
10.Tab.Dolo650mg po/tid
.Monitor vitals-4rth hourly
I/O charting
Planning for discharge